



Paraplegia rehabilitation is among the most demanding and most misunderstood areas of post-acute care. Patients and families come to it carrying two opposing fears: that nothing meaningful can be achieved or that with enough effort, full walking recovery is inevitable. Neither is accurate and both misunderstandings cause real harm – one by leading families to abandon rehabilitation before its benefits are realised, the other by creating expectations that, when unmet, are experienced as failure. What modern paraplegia rehabilitation actually achieves sits between these extremes, and it is considerably more than most families are told at the point of spinal cord injury diagnosis.
What Paraplegia Actually Means Clinically
Paraplegia refers to the loss of motor and sensory function in the lower body, caused by injury or damage to the thoracic, lumbar, or sacral segments of the spinal cord. It is distinct from tetraplegia which involves all four limbs. The extent of impairment depends on the level and completeness of the injury. A complete injury means no motor or sensory function is preserved below the injury level. An incomplete injury means some function remains and this distinction is clinically significant because it determines the realistic scope of rehabilitation goals.
Incomplete spinal cord injuries, which account for a substantial proportion of cases, carry meaningful potential for functional recovery that extends well beyond what was once considered possible. The spinal cord’s capacity for neuroplasticity (the reorganisation of neural pathways in response to stimulation) has changed the rehabilitation landscape dramatically over the past two decades.
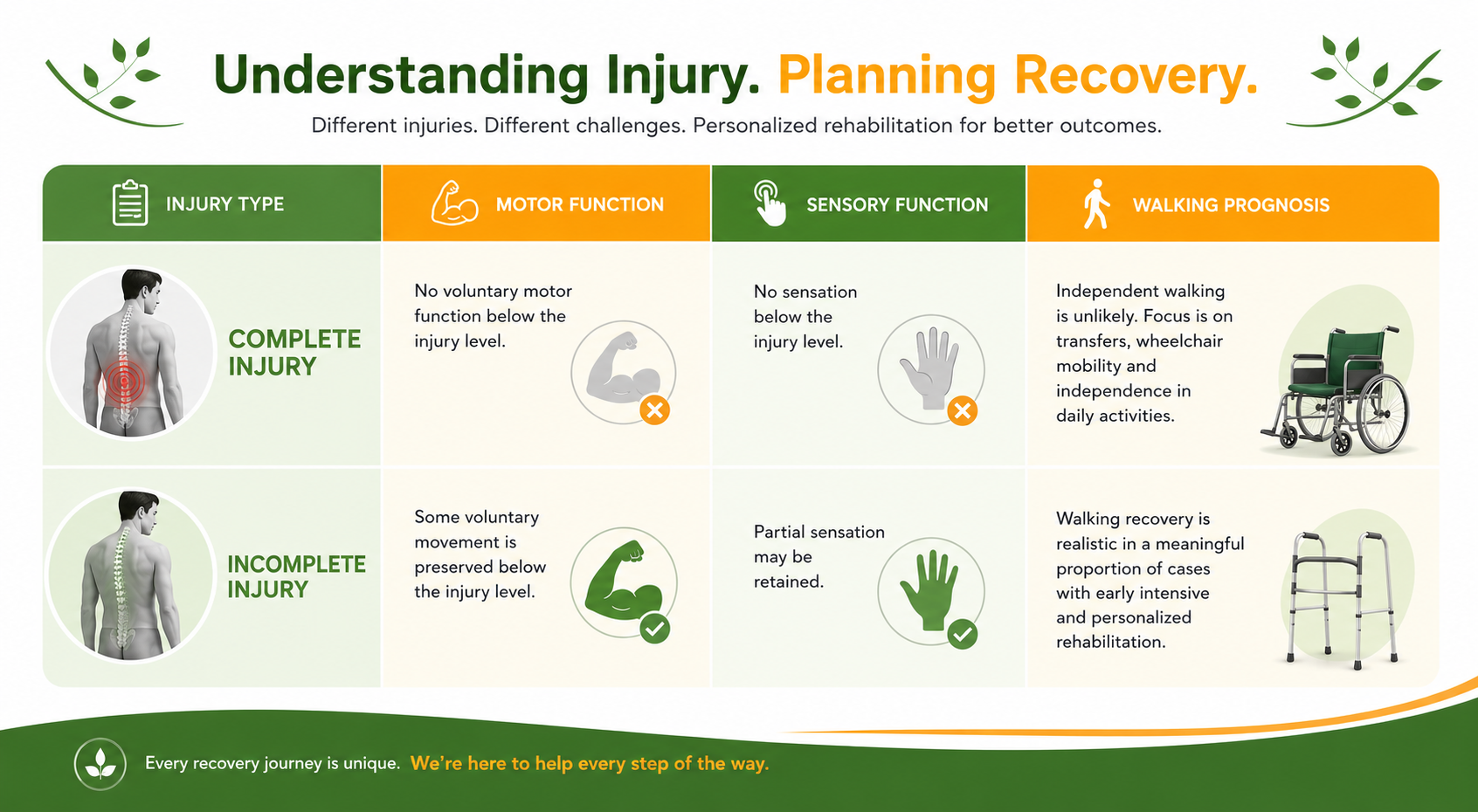
Injury Type | Motor Function | Sensory Function | Walking Prognosis |
Complete Injury | No voluntary motor function below injury level | No sensation below injury level | Independent walking unlikely; functional goals focus on transfers, wheelchair mobility and self care. |
Incomplete Injury | Some voluntary movement preserved below injury level | Partial sensation may be retained | Walking recovery realistic in a meaningful proportion of cases with early intensive rehabilitation |
Why Paraplegia Rehabilitation Has Changed
Spinal cord injury rehabilitation in Bangalore and across major Indian cities has evolved considerably from the historical model of passive management and assisted transfer training. The shift has been driven by a clearer understanding of how the injured spinal cord responds to training.
The nervous system does not simply repair itself after injury. But it does adapt, reorganise, and recruit alternative pathways when those pathways are consistently activated through purposeful movement. This is the principle that underpins modern neuro rehabilitation approaches – that walking again, or regaining meaningful lower limb function, depends not on waiting for the cord to heal but on driving neuroplastic change through repetitive, task-specific training initiated as early as medically possible.
Physiotherapy rehabilitation for paraplegia now integrates robotic-assisted gait training, body-weight-supported treadmill therapy, functional electrical stimulation and intensive manual therapy in ways that were not clinically available a generation ago. The evidence base supporting these approaches has grown substantially and outcomes for patients who receive early, intensive, structured rehabilitation are consistently better than those who do not.
Modern Paraplegia Rehabilitation: Key Advances
Robotic assisted gait training – allows repeated, precisely controlled stepping practice even where voluntary leg movement is minimal
Body-weight-supported treadmill therapy – enables upright gait training with reduced load, activating spinal circuits that drive neuroplastic reorganisation
Functional electrical stimulation – delivers targeted electrical impulses to paralysed muscle groups to produce purposeful contraction
Neuroplasticity-based protocols – intensive, task-specific training programmes designed to exploit the injured cord’s capacity to adapt
Early mobilisation pathways – structured mobilisation from the acute phase onward, preventing secondary complications that compromise later rehabilitation
Can Patients with Paraplegia Walk Again?
This is the question families ask first and it deserves a direct answer. For complete injuries at higher thoracic levels independent functional ambulation remains unlikely with current technology. This is a clinical reality that rehabilitation teams communicate honestly, because setting an unachievable walking goal and pursuing it exclusively comes at the cost of functional goals that are achievable and that make a genuine difference to quality of life.
For incomplete injuries – particularly those at lower thoracic and lumbar levels – walking recovery is a realistic goal in a meaningful proportion of cases. The degree of recovery achieved depends on the severity and level of the injury, the time elapsed before rehabilitation began, the intensity and consistency of the rehabilitation programme, and the patient’s age and overall health. Patients who begin structured spinal cord injury rehabilitation in Bangalore or other specialist centres early, and who sustain it over the required timeframe, achieve outcomes that frequently exceed initial projections.
Walking, however, is not the only meaningful outcome of paraplegia rehabilitation and for some patients, it is not the most important one. Independent transfers, wheelchair mobility, pressure care management, bladder and bowel function, pain management, and psychological adaptation to life post-injury are all rehabilitation goals with profound implications for independence and dignity. A patient who cannot walk independently but can transfer safely, manage their own care, and live outside a hospital environment has achieved something that requires the same clinical investment as walking recovery.
If you or your loved one is planning for paraplegia rehabilitation our Sukino Healthcare provides specialist spinal cord injury rehabilitation in Bangalore, combining physiotherapy rehabilitation, neuro rehabilitation, occupational therapy, and medical management within a structured inpatient programme. Early intervention produces measurably better outcomes. Contact Sukino’s rehabilitation team to learn more. |
What a Comprehensive Paraplegia Rehabilitation Programme Involves
Neuro rehabilitation for spinal cord injury is not a single intervention – it is a coordinated programme delivered by a multidisciplinary team across an extended timeline.

Programme Component | What It Addresses |
Physiotherapy Rehabilitation | Strengthening of preserved muscles, spasticity management, gait training, transfer training & functional mobility |
Occupational Therapy | Activities of daily living retraining, adaptive equipment, home modification and return-to-work planning |
Neuro Rehabilitation | Task-specific training, robotic-assisted gait, body weight supported treadmill, functional electrical stimulation |
Bladder & Bowel Rehabilitation | Catheterisation training, bowel management, prevention of UTIs and complications from neurogenic bladder |
Spasticity & Pain Management | Medication review, positioning, physical modalities, and injections where indicated |
Psychological Rehabilitation | Grief processing, adjustment counselling, family support – directly correlated with better functional outcomes |
What Families Are Often Not Told About Spinal Cord Injury Rehabilitation
The completeness of the injury matters more than the injury level alone – an incomplete injury at a high level may have better walking potential than a complete injury at a lower level.
Secondary complications – pressure injuries, recurrent UTIs, spasticity – are not inevitable. They are largely preventable with appropriate rehabilitation management.
Psychological support is not optional in spinal cord injury rehabilitation. Adjustment to paraplegia involves a grief process that directly affects physical rehabilitation outcomes when unaddressed.
Long-term follow-up is a clinical necessity not a precaution. Needs change as years pass, and periodic reassessment prevents manageable problems from becoming serious ones.
The Role of Timing in Spinal Cord Injury Rehabilitation
The timing of rehabilitation initiation has a direct and measurable effect on outcomes. Early mobilisation (as soon as the injury is medically stable) prevents the secondary complications that compound the primary injury: pressure injuries, deep vein thrombosis, muscle atrophy, contracture, pneumonia and the psychological deterioration that comes with prolonged inactivity in an acute hospital setting.
Families are sometimes advised or choose to wait until the patient is more stable before beginning rehabilitation. The window during which neuroplastic change is most responsive to intervention is concentrated in the early post injury period. Delayed rehabilitation does not simply push the same outcomes. Rather it forecloses some of them.
Life Beyond the Rehabilitation Centre
The goal of paraplegia rehabilitation is not to produce a patient who performs well in a clinical setting. It is to produce a patient who lives well outside one. For many patients, this means reintegration into family life, return to meaningful occupation, and management of the long-term health consequences of spinal cord injury – which, without active prevention, include repeated urinary tract infections, pressure injuries, chronic pain, and the cardiovascular complications of a sedentary lifestyle.
Long-term follow-up with a spinal cord injury rehabilitation team is not a luxury – it is a clinical necessity. The work done in the initial rehabilitation period establishes a baseline but maintaining and building on that baseline requires ongoing professional support and periodic reassessment as the patient’s needs evolve over years.


