



Guillain-Barré syndrome treatment in India has improved substantially over the past decade, but what happens after the acute phase – the weeks and months of rehabilitation that determine how fully a patient recovers is poorly understood by most families at the point of diagnosis. GBS is not a condition where treatment ends when the hospital does. The acute interventions stabilise the nervous system; rehabilitation is what restores life.
The reason every GBS patient needs a personalised rehabilitation plan is not clinical formality. It is because no two cases are alike. The rate of onset, severity, degree of respiratory involvement, specific pattern of nerve damage, and the patient’s age and baseline fitness all combine to produce a recovery trajectory that cannot be mapped onto a generic template. A plan built on averages fails the patient who falls outside them – and in GBS, most patients fall outside the average in some clinically significant way.
What GBS Does to the Body and Why Recovery Is Complex
Guillain-Barré syndrome is an autoimmune condition in which the immune system attacks the peripheral nervous system, damaging the myelin sheath and in more severe cases, the axons themselves that allow nerves to transmit signals to muscles. The result is a rapidly progressive, ascending weakness that can reach its worst point within days to weeks & in severe cases requires ventilatory support.
The recovery process reverses this progression, but slowly and unevenly. Myelin regrowth happens at approximately one millimetre per day, meaning nerve pathways disrupted in the lower limbs may take many months to regenerate sufficiently to support functional movement. In cases of axonal involvement, recovery is slower and some residual deficits may be permanent.
Fatigue is one of the most underestimated features of GBS recovery. It is neurological in origin rather than simply physical deconditioning and it does not respond to rest the way ordinary tiredness does. Many patients who appear to be progressing well in structured sessions experience profound exhaustion afterwards that takes hours to resolve. A rehabilitation plan that includes built-in rest periods, pacing activity carefully, and adjusting session intensity to the patient’s energy on a given day will produce a patient who improves in the clinic but deteriorates at home.
When GBS Rehabilitation Needs Immediate Clinical Attention
- Worsening weakness or new loss of function after a period of stability – may indicate a relapse or a secondary complication
- Increasing breathlessness or inability to take a full breath – respiratory muscle compromise requires urgent review
- Severe autonomic symptoms: fluctuating blood pressure, heart rate irregularities, urinary retention
- Neuropathic pain that is worsening or uncontrolled – signals that the current management plan needs revision
- Marked deterioration in mood or emergence of suicidal ideation – psychological support should be integrated into the plan.
Why a Generic Rehabilitation Plan Does Not Work for GBS
GBS recovery is sufficiently variable that a standard rehabilitation pathway provides only a partial framework. The relevant variables are numerous: which nerve groups are most affected, whether autonomic involvement is present, the severity of residual pain, the degree of sensory loss versus motor loss and the psychological impact of what is, for many patients, a sudden and terrifying loss of control over their own body.
A personalised rehabilitation plan for GBS begins with a thorough functional assessment – not at acute hospital discharge, but at admission to the rehabilitation programme and repeatedly thereafter. It maps current motor function joint by joint, identifies sensory deficits that affect balance independently of strength, assesses fatigue severity, screens for anxiety and depression (both substantially elevated in GBS) and evaluates the home environment and social support available after discharge.
From this assessment, realistic, staged goals are established and reviewed regularly because GBS recovery does not follow a linear trajectory and a plan that worked in week four may need significant revision by week eight.
If you or your family member is considering Guillain-Barré syndrome treatment in India, Sukino Healthcare provides personalised Guillain-Barré syndrome rehabilitation in Bangalore combining physiotherapy, fatigue management, neuro rehabilitation, and medical oversight within a structured inpatient programme tailored to each patient’s specific recovery trajectory. Contact our clinical team to learn more. |
GBS Recovery Timeline Week by Week
GBS recovery follows three phases: onset to the peak, the plateau at maximum weakness, and the recovery phase – which is itself heterogeneous and extends over months to years.
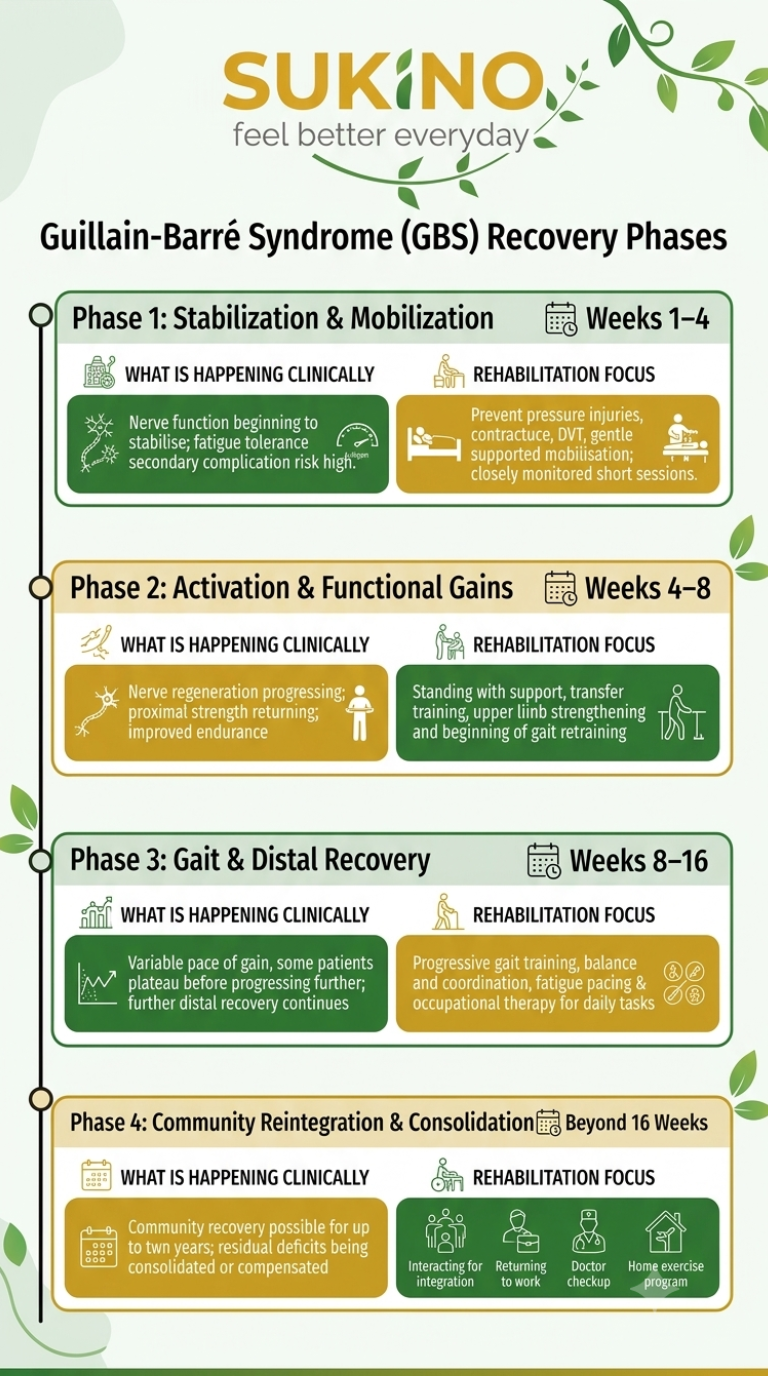
Phase / Timing | What Is Happening Clinically | Rehabilitation Focus |
Weeks 1–4 | Nerve function beginning to stabilise; fatigue tolerance minimal; secondary complication risk high. | Prevent pressure injuries, contracture, DVT; gentle supported mobilisation; closely monitored short sessions. |
Weeks 4–8 | Nerve regeneration progressing; proximal strength returning; improved endurance | Standing with support, transfer training, upper limb strengthening and beginning of gait retraining |
Weeks 8–16 | Variable pace of gain; some patients plateau before progressing further; distal recovery continues | Progressive gait training, balance and coordination, fatigue pacing & occupational therapy for daily tasks |
Beyond 16 Weeks | Continued recovery possible for up to two years; residual deficits being consolidated or compensated | Community reintegration, return to work, long-term follow up, home programme maintenance |
What Families Are Often Not Told About GBS Recovery
- A plateau in progress is a normal clinical feature of nerve regeneration, not evidence that rehabilitation has stopped working or that no further recovery is possible.
- Many patients experience their most significant functional gains well past the twelve-week mark – GBS recovery timelines regularly extend to one to two years.
- Residual fatigue can persist long after strength appears to have returned, and this affects return to work and daily function in ways that are not always taken seriously without clinical validation.
- Psychological impact of GBS is substantial and frequently under-treated – anxiety and depression in GBS recovery are clinical problems that affect physical rehabilitation outcomes when left unaddressed.
The Components of Personalised GBS Rehabilitation
Neuro rehabilitation for GBS is not a single intervention – it is a coordinated programme delivered by a multidisciplinary team, with the components and their weighting adjusted to each patient’s specific presentation.

Rehabilitation Component | What It Addresses in GBS |
Physiotherapy | Motor recovery, gait retraining, balance, strength – responding to the variable pattern of return across muscle groups |
Occupational Therapy | Adaptive self-care, hand function retraining, home assessment, return to work planning |
Fatigue Management | Structured pacing, education about neurological fatigue & strategies for sustaining activity across the full day |
Pain Management | Neuropathic pain specific to GBS – pharmacological and non-pharmacological approaches integrated into the plan |
Respiratory Physiotherapy | For patients with ventilator history or residual respiratory muscle weakness – breathing exercises, secretion clearance |
Psychological Support | Adjustment to sudden severe illness, anxiety management, family counselling – correlated with better functional outcomes |
Why Timing and Setting Both Matter
Paralysis rehabilitation for GBS produces better outcomes when it begins early and is delivered in a structured inpatient environment for the initial intensive phase. Patients who begin inpatient neuro rehabilitation immediately following acute hospital discharge, rather than waiting weeks for any structured programme to begin, consistently show superior functional outcomes.
The setting matters because GBS rehabilitation requires daily neurological monitoring, the ability to adjust programme intensity in real time and clinical coordination between physiotherapy, occupational therapy, respiratory support, and medical management that is difficult to replicate through outpatient or home-based care alone in the early stages.
For families who are considering neuro rehabilitation in Bangalore, Kochi, Hyderabad, and Kozhikode choosing a centre that offers early, multidisciplinary rehabilitation can make a meaningful difference in recovery. Beginning rehabilitation at the right time and in the right setting helps maximise functional improvement and supports a smoother return to daily life.


