



Most families assume that leaving the intensive care unit means the hard part is over. In clinical terms, the opposite is closer to the truth. The ICU saves lives – it stabilises the critically ill, manages life-threatening organ failure, and buys the time that recovery requires. What it cannot do, within the constraints of its own environment and purpose, is rebuild what critical illness has taken from the body. That work belongs to long term acute care services and it begins not after discharge from hospital but during the transition out of the ICU itself.
Post-ICU recovery is now understood as a distinct clinical entity. Patients who survive critical illness whether from sepsis, respiratory failure, cardiac events, traumatic injury, or major surgery carry a burden of physical, cognitive and psychological impairment that persists long after the acute threat has passed. This constellation has a name in the clinical literature: Post-Intensive Care Syndrome, or PICS. It is common, it is severe and it is almost entirely undertreated in the Indian post-acute care system.
What Happens to the Body in the ICU
The ICU environment, despite its clinical necessity, is physiologically hostile in ways that accumulate over time. Prolonged bed rest produces muscle loss at a rate of two to five percent per day in ICU patients. A patient who spends two weeks in the ICU may lose a quarter of their muscle mass. This is not ordinary deconditioning – it is ICU-acquired weakness, a distinct syndrome affecting respiratory muscles, limb muscles and the neuromuscular junctions responsible for movement. It does not reverse with time or rest alone.
Sedation, while essential for ventilated patients, disrupts sleep architecture, impairs cognitive recovery and contributes to the confusion that characterises post-ICU delirium – a condition affecting the majority of ventilated patients and associated with cognitive impairment that can persist for months or years.
Respiratory function, even in patients who did not require mechanical ventilation, is compromised after an ICU admission. Diaphragmatic weakness, reduced lung compliance and impaired secretion clearance create a respiratory burden that ordinary activity exposes immediately.
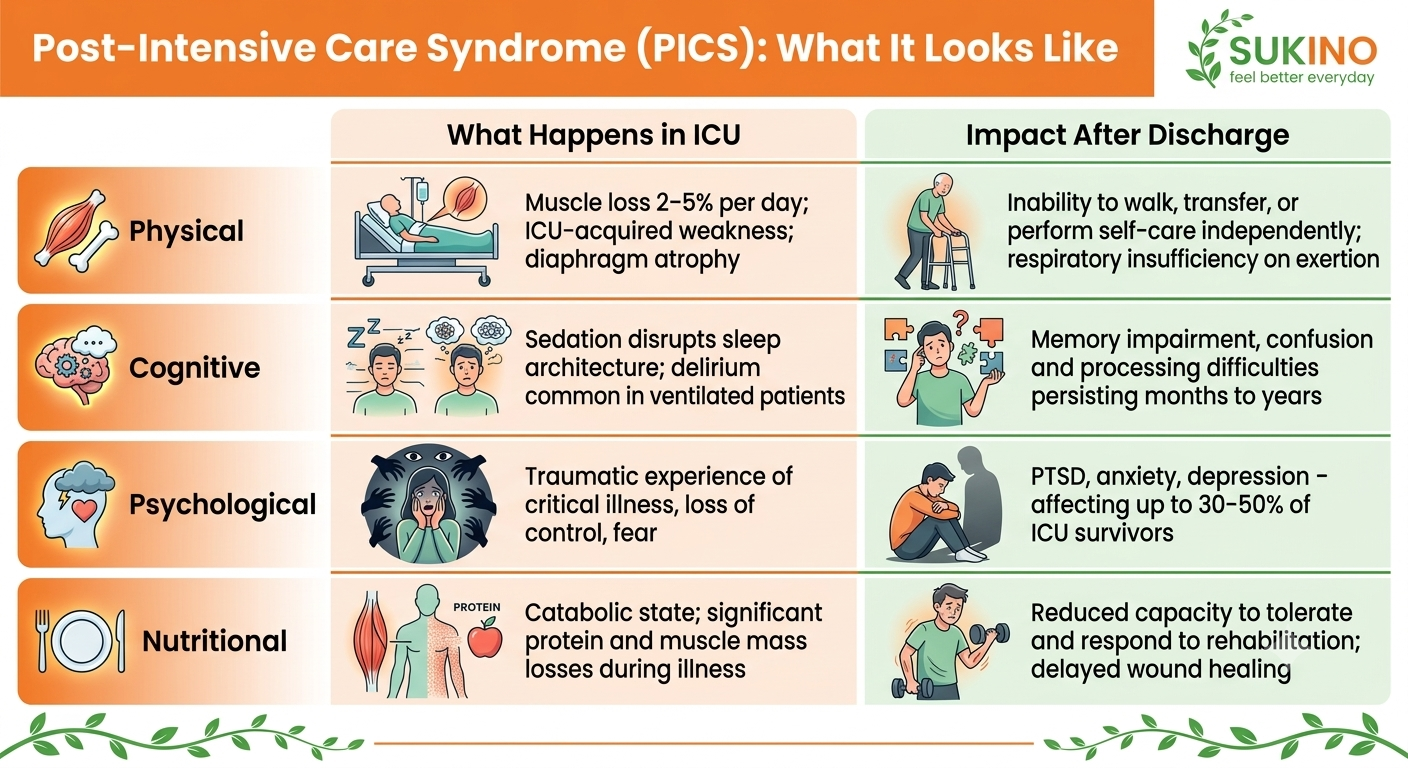
Post-Intensive Care Syndrome: What It Looks Like
Domain | What Happens in ICU | Impact After Discharge |
Physical | Muscle loss 2–5% per day; ICU-acquired weakness; diaphragm atrophy | Inability to walk, transfer, or perform self-care independently; respiratory insufficiency on exertion |
Cognitive | Sedation disrupts sleep architecture; delirium common in ventilated patients | Memory impairment, confusion and processing difficulties persisting months to years |
Psychological | Traumatic experience of critical illness, loss of control, fear | PTSD, anxiety, depression – affecting up to 30–50% of ICU survivors |
Nutritional | Catabolic state; significant protein and muscle mass losses during illness | Reduced capacity to tolerate and respond to rehabilitation; delayed wound healing |
Warning Signs That Post-ICU Recovery Needs Urgent Clinical Review
Warning signs are:
- Worsening breathlessness at rest or with minimal activity after ICU discharge
- Oxygen saturation dropping below 94% with light exertion or movement
- New or increasing confusion, disorientation, or inability to recognise familiar people
- Inability to stand or walk that is not improving or deteriorating beyond two weeks post-discharge
- Wound dehiscence, fever, or signs of infection at any surgical or access site
- Complete absence of appetite persisting beyond one week after discharge
Why Long-Term Acute Care Services Bridge the Gap
Long term acute care services (LTACs) exist precisely because the gap between ICU discharge and home is too wide for most critically ill patients to cross safely without structured clinical support. The acute hospital’s mandate is stabilisation. The home environment’s capacity for complex clinical management is limited. LTACs occupy the clinical space in between: providing the medical monitoring, respiratory rehabilitation and nutritional management that critically ill patients require as they move out of the acute phase.
This is not step-down care in the sense of reduced intensity. For many post-ICU patients, the clinical demands of the early recovery period are substantial – ongoing ventilatory weaning, wound management, nutritional support for a body that has been in catabolic crisis and daily rehabilitation dosed carefully to produce benefit without inducing post-exertional deterioration.
Families who bring a post ICU patient home without this intermediate clinical layer often find themselves managing a situation they are not equipped for: a person who cannot walk safely, whose breathing becomes laboured with minimal exertion, who is confused & frightened and whose medical needs exceed what family support alone can manage safely.
If you or your loved one is searching for rehanilitation after an ICU discharge Sukino Healthcare provides long term acute care services (LTAC) and post-hospital rehabilitation for post-ICU patients in Bangalore – combining respiratory rehabilitation, physical rehabilitation, nutritional support, and 24-hour medical monitoring within a structured inpatient programme. Speak with our team before ICU discharge to plan the right next step. |
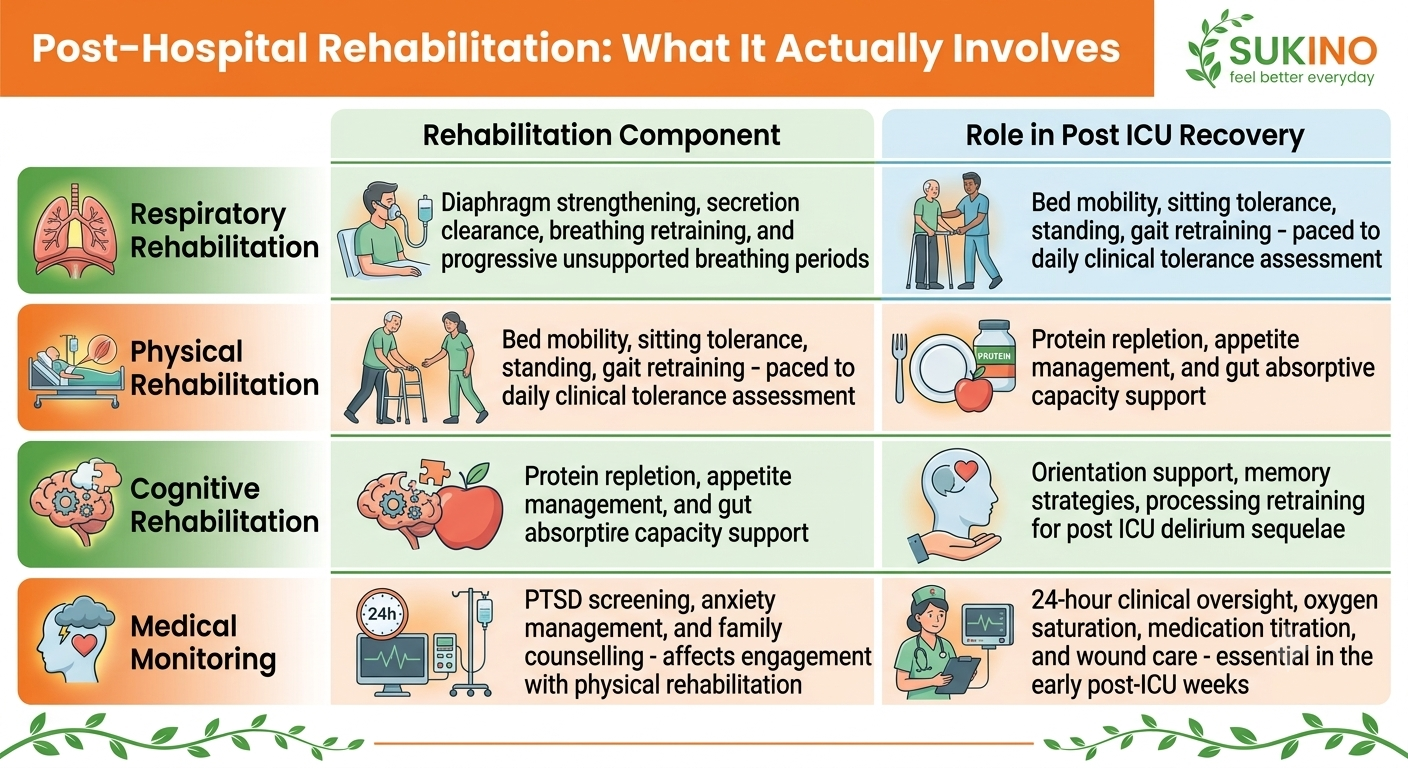
Post Hospital Rehabilitation: What It Actually Involves
Rehabilitation Component | Role in Post ICU Recovery |
Respiratory Rehabilitation | Diaphragm strengthening, secretion clearance, breathing retraining and progressive unsupported breathing periods |
Physical Rehabilitation | Bed mobility, sitting tolerance, standing, gait retraining – paced to daily clinical tolerance assessment |
Nutritional Rehabilitation | Protein repletion, appetite management and gut absorptive capacity support |
Cognitive Rehabilitation | Orientation support, memory strategies, processing retraining for post ICU delirium sequelae |
Psychological Support | PTSD screening, anxiety management and family counselling – affects engagement with physical rehabilitation |
Medical Monitoring | 24-hour clinical oversight, oxygen saturation, medication titration and wound care – essential in the early post-ICU weeks |
ICU at Home Services in Bangalore: When It Is and Is Not Appropriate
ICU at home service in Bangalore has expanded significantly, and for the right patient it provides a genuine pathway for those who do not need inpatient monitoring but whose medical needs exceed what standard community care can manage. Patients who are medically stable, have adequate home environments, and have family members who can be trained may be suitable candidates.
However, ICU at home is not appropriate for patients who still require ventilatory weaning, have complex wound management needs, need daily medication titration for haemodynamic stability, or present with the degree of weakness and cognitive impairment that makes safe home mobility a realistic risk. For this group, long term acute care services in a structured inpatient environment remain the clinically appropriate step.
What Families Should Ask Before ICU Discharge
Before a family member is discharged from an ICU in Bangalore or anywhere in India, four questions should be asked: Is respiratory function genuinely stable, or still variable? What is the current level of functional independence – can the patient walk, transfer and manage basic self-care? Has cognitive function been formally assessed? And what medical monitoring will be needed in the first two to four weeks?
The answers determine whether the appropriate next step is home, ICU at home support, LTAC services or further inpatient rehabilitation. Asking these questions before discharge rather than after a failed home care attempt is the decision that changes outcomes.


